(2013) Looks Could Kill (12 page)
“Is it alright if I call you Brian?” she asked. “My name is Emma, by the way. I’m interested in knowing more about you and what the pain means for you. I may be wrong, but I get the feeling that there’s something more than the pain which keeps you going. Am I right?”
“It’s funny, doctor,” he said, “but I was thinking just the same when I was waiting for the clinic to start. I may have lost my wife, but since she passed on I’ve discovered I enjoy cooking and if I’m not watching cookery programmes I’m busy on the stove. And then there’s my cat Lucy who’s a real comfort when the pain gets too much.”
“We often joke about pet therapy but it works for some,” said Emma. “And cooking sounds an excellent hobby. Do you enjoy eating what you cook?”
“You’ve hit the nail on the head, doctor,” he said. “My appetite isn’t so good and then there’s the constipation.”
“I think we could do something about that,” said Emma. We could change your medication and get a dietician to help you prepare food that would stimulate your appetite and your bowels. How does that sound?”
Emma filled in a prescription for the pharmacy and gave it to her patient. “You try that rather than what you were on before and ask the receptionist to book you in next week. And I’ll try to get you an appointment with the dietician at the same time. Take care of yourself and give Lucy a stroke from me.”
Brian laughed and thanked her, making his way slowly out of the room. Yes, there’s something there, Emma thought, but he’s still struggling.
Her next patient was a follow-up: someone seen by the physiotherapist who’d asked for advice on alternatives to analgesics. Emma agreed with her colleague that acupuncture would be worth trying. She found her acupuncture set and inserted some needles into some local points. She left the patient lying down in her consulting room and said she’d be back in ten minutes or so.
Emma found the team discussion useful. She discovered that they were all quite like-minded and there was no particular jarring note. She thought this was a team she could work with. But she also got the impression that they’d leave no stone unturned, which might mean going too far and possibly causing more distress. That’s something she’d have to watch out for.
December 2000, Christmas Eve
Two middle-aged men sat in a comfortable, book-lined room enjoying single malt whiskies in front of a log fire. They had copies of a brown, foolscap file on their laps.
“Definite potential here, I think. Do you have anything else, you know, reading between the lines?” asked the first man.
“Well, she’s an only child for a start. Unstable start in life, conflicts with religion and a certain propensity for unorthodox retribution. A brief dalliance with the law following some, er, voluntary work in a nursing home, clear evidence of a certain ability to relieve suffering and also a tendency to use the blade on herself. Impressive Oxford interview but a little economical with the truth. A largely unremarkable undergraduate career with a hobby of butterfly collecting courtesy of our Mrs Brown. I believe she met our friend Cuthbert at one point. Solid junior doctor with a few unexpected deaths - if you catch my drift - then trained in pain medicine. Now a NHS consultant, well respected although hardly of international repute yet,” said the second.
“And presently single,” said the first.
“Indeed, still the amateur rather than the virtuoso,” said the second.
“We shouldn’t risk her doing anything, er, precipitous,“ said the first.
“Indeed, no rush, I think,” said the second.
They finished their single malt whiskies and moved on to the next file.
September 2001
From time to time, Emma had plans to get involved in research projects, although work invariably got in the way. As a registrar, she had a publication on some work she did on pain perception, but that seemed a long time ago. She thought she should start thinking about a research project she could do now, and so she approached a colleague called Michael Moore who was up at Oxford with her and now worked as a consultant radiologist in the imaging department. Emma had also received a recent reminder from him about a reunion for the 1981 cohort of medical students.
“Hi, Michael, it’s Emma Jones here. You probably don’t remember me, but I was up at Oxford between 1981 and 1986 and we shared a dissecting table.”
“Gosh, yes, the butterfly girl. How are you doing?”
“I’m good. I got a consultant job in pain medicine six years ago. No major hiccups so far, although I’m not looking forward to appraisal and all that sort of thing.”
“Me neither.” He laughed. “Emma, I’m guessing this isn’t a social call; is there anything I can help you with?”
“Well, yes there is. I’ve been thinking about getting a research project going and something along the lines of functional MRI of patients with chronic pain and various interventions seems a possibility. Is there any chance I could come and have a chat?”
“That does sound interesting and it’s not a million miles away from something we’re doing ourselves on perception. I tell you what: you come to imaging and offer to be a test subject and I’ll buy you lunch. How about 12 next Monday?”
“Sounds good. I’ll make sure I’ve removed any jewellery.”
And so Emma pitched up at imaging at the appointed time. She’d put together a rough draft of a research proposal over the weekend for Michael to look through. She’d also read up on MRI scanning and it all sounded very cutting edge; fMRI or functional MRI was clearly going to be the next step in discovering how the brain really works, although the equipment was fiendishly expensive and a danger if anything metallic was brought near it.
The MRI scanner itself is seriously impressive and it’s not ideal for someone who suffers from claustrophobia; think of putting your head in a giant, loudly-clicking washing machine and you’ll get the idea of what it’s like.
Michael’s study was being done in conjunction with psychologists who were interested in seeing whether the brain processes images of people differently according to age, sex, skin colour and various other characteristics. All Emma had to do was lie on the movable couch with her head in the scanner and concentrate on various photos that would be handed to her in turn. She also had to complete a questionnaire which asked various searching questions, including about sexuality. And there was the usual consent form.
The clicking that the scanner made was off-putting, but Emma managed to block that out to concentrate on the photos. And they certainly were varied: young and old, clothed and naked, standing up and lying down, and much more besides.
After about an hour, Emma was extracted from the scanner and went through to the control room to hear about the results from Michael.
“Well, strictly speaking, Emma, we’re not really meant to divulge the results to subjects, but there’s something rather interesting that came up on your scans.”
“That sounds ominous, Michael, it’s nothing bad, is it?”
“No, Emma, I can assure there’s no space occupying lesion or anything like that. On the contrary, what we’re seeing is activation in parts of your brain that’s really off the scale; in fact, I’ve never seen anything like it before. See, have a look here.”
Emma looked at the monitor, trying to decipher what she could see. She was also desperately trying to recall her neuroanatomy lectures in order to avoid saying the wrong thing. What she could see were some intensely bright areas in the region she recognised as the cortex.
“Okay, I take it that the bright area there is activation – that’s the correct word, isn’t it – and that must be the visual cortex.”
“Yes, all correct, but if you look here – this is the limbic system, by the way – you can see that there’s activation there as well, which might be your emotional response to what you’re looking at. Now, if I change the scan to when you were looking at some of other images, you can see the huge difference between the two scans.”
“Yes, I can see that. Do you get that big difference with other subjects?”
“No, nothing like that, just small differences. You know, straight men getting more activation when they look at a naked woman than a naked man, or variations on that, but no big differences like yours. And we don’t usually see all that limbic activation.”
“So, what’s making my brain activate like that?”
“Well, that’s the funny thing, it seems to be images of older people and there’s no difference between sexes, or whether they standing up or lying down; just the simple fact that they’re old. I don’t suppose you’re a closet gerontophile or something?”
“Thanks Michael, but I’m definitely not!”
“Anyway, it’s very interesting whatever it is, but perhaps we ought to go and have lunch before the canteen closes and then talk about your research proposal.”
Lunch with Michael was pleasant enough and he turned out be rather more personable than when she knew him at Oxford. Their discussion about a research project was also helpful, although she knew that getting anything off the ground would take months of applications to the hospital ethics committee with no guarantee of getting it signed-off. She also couldn’t stop thinking about the scan results; she certainly hadn’t anticipated anything unusual being found when she volunteered.
Returning to her office, she started jotting a few thoughts down on paper:
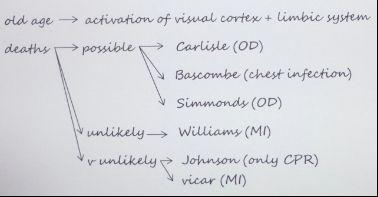
Emma decided she needed to construct a hypothesis. Let’s suppose that somehow she could influence the health of people in some way – for instance, make someone take an overdose, have an MI or develop a chest infection. If she could do that, what would be the process involved? Could it be connected with the scan result that showed that her brain got hyper-activated by looking at older people? It sounded strange, but would provide a commonality with Carlisle and Bascombe where she recalled a very strong emotional feeling when she looked at them. Emma thought that might also be the case with Simmonds where she experienced the strongest emotional feeling ever; and he was also the most unwell. That might be a factor. But with younger patients like Williams, Emma didn’t experience any emotional feeling apart from sadness because he was so young. Emma thought that the vicar was probably a coincidence given that she barely had a functioning CNS then. But if all this was something connected with a sort of hyper-activation of parts of the brain, how could this actually cause something to happen to other people?
For Emma, this was where the hypothesis totally fell apart and started entering the realms of the X-Files. Perhaps she should call in Mulder & Scully. She was also feeling increasingly uncomfortable with the idea that she was some sort of modern-day Medusa. She felt that she needed to run this by somebody, although she was struggling to think who it should be. Clearly not someone connected with the General Medical Council, unless she wanted to get struck off the medical register.
But one thing she needed to check with Michael was whether her response on the scans was more about illness than age. She phoned him in his office.
“Hi, Michael, it’s Emma. Have you got a minute? I just wondered whether you could check the scans you did on me and see whether there’s any difference in the results according to the sort of older patient; you know, lying in bed or on a trolley, or not.”
“Okay, Emma, I think I can do that if you were shown the right images. I’ll give you a ring back in a few minutes.”
“Thanks, Michael, I’d appreciate that.”
Ten minutes later, Michael rang back.
“Emma, it’s strange, the activation was off the scale for old people whose photos showed them lying down; as if they were ill in other words. And there was something else too: certain photos we showed you could have been perceived as images of people in pain, and those scans showed activation in the prefrontal, insula and anterior cingulate. It’s weird but it’s almost as if you were experiencing their pain just by looking at the photos.”
“Michael, I think I need to see you again.”
And so, for the second day in a row, Emma visited the imaging department, but this time she chose to talk in his room rather than anywhere more public.
“You look worried, Emma,” said Michael.
“I am, Michael. Now, I know what I’m going to tell you is going to sound screwy, but it’s something I’ve got to say someone, or else I’ll go completely out of my mind. So please hear me out.”
Emma pulled out the piece of paper with her jottings on it and started going through the associations that she’d been making.
“But the difficulty is that any temporal connection seems to be all over the place – sometimes virtually immediate in the cases of Carlisle and Simmonds, but sometimes weeks later in the case of Bascombe - and then there are the emotions I get, which can range from just a feeling in the case of Bascombe to a huge wave that left me drained in the case of Simmonds. It’s very confusing. What do you think, Michael?”
He leant back in his chair to think and then sat forward, looking in her eyes. “Have you considered seeing a psychiatrist, Emma?”
“Oh god, I thought you’d say something like that! Look, Michael, I’m sure something is happening and that I’m connected with it and I need to understand what it is.”