i bc27f85be50b71b1 (17 page)
Read i bc27f85be50b71b1 Online
Authors: Unknown
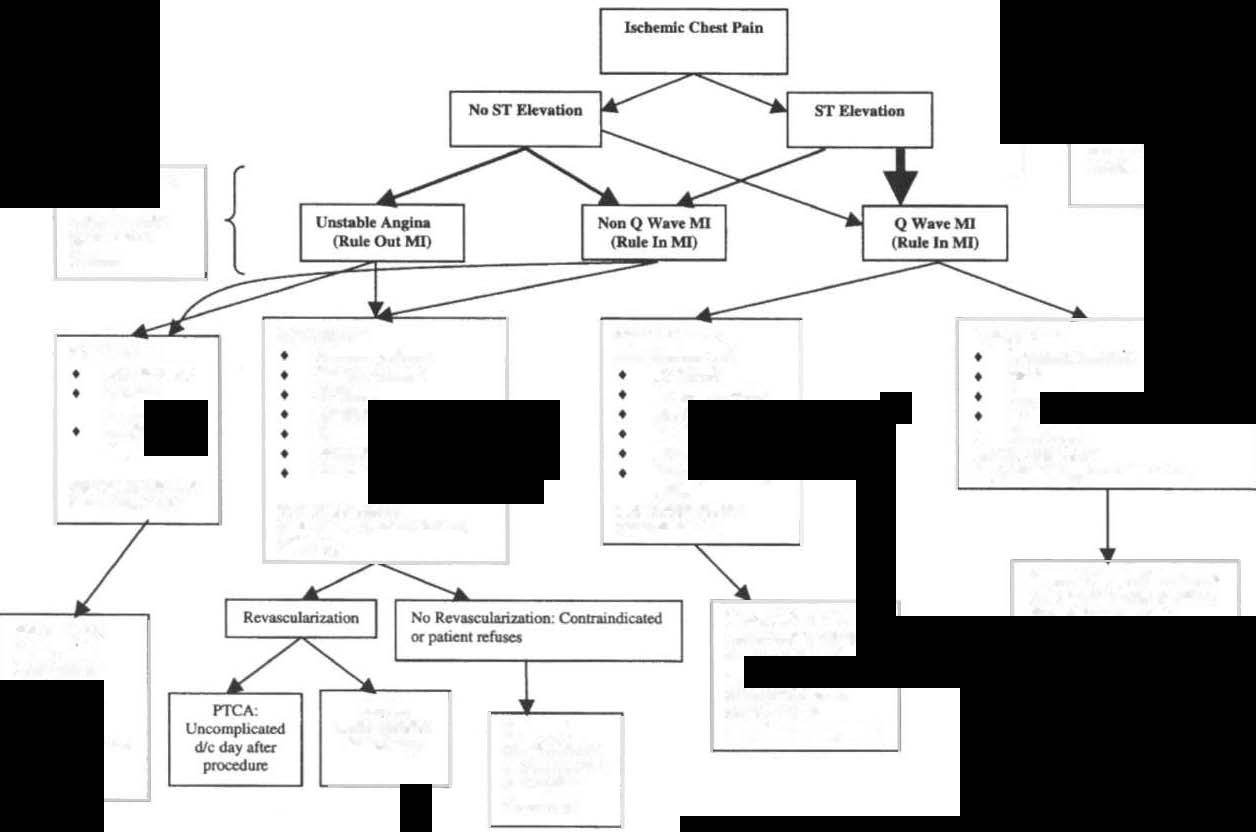
1-9 provides a schemaric of possible clinical courses for parients
admirred wirh chesr pain.

CARDIAC SYSTEM
4 1
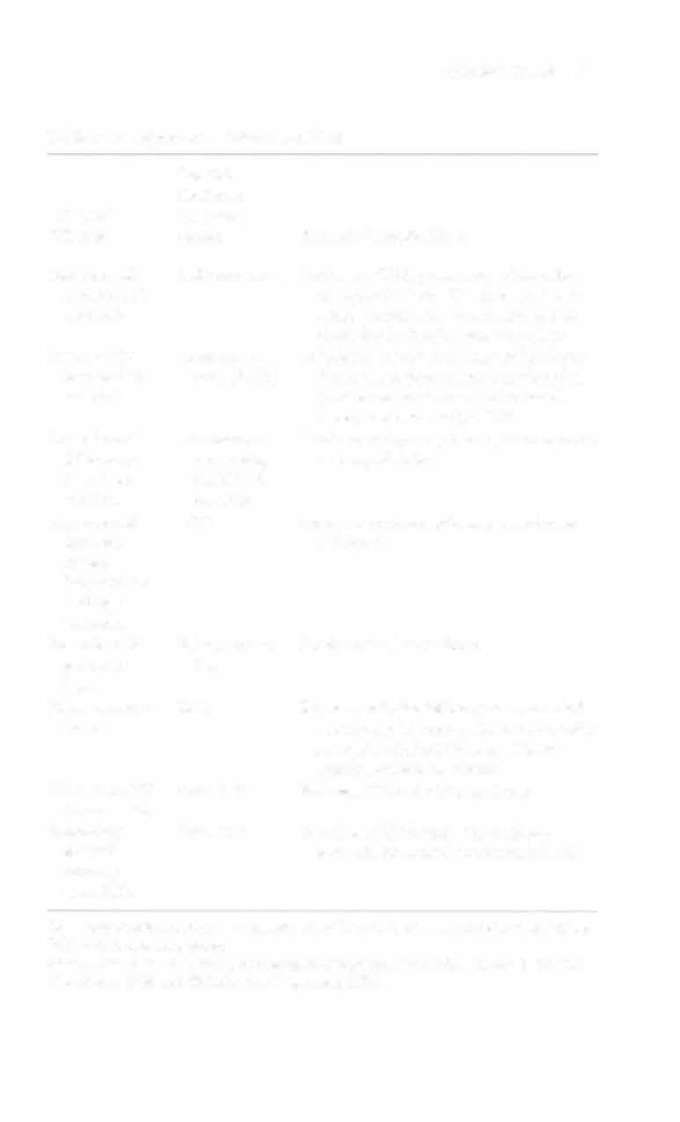
Table I-B. Myocardial lnfarcrions (MIs)
Possible
Occluded
Ml/Wall
Coronary
Affecred
Artery
Possible Complications
Anterior MY
Left coronary
Left-sided CHF, pulmonary edema, bunanterior left
dle branch block, AV block, and venventricle
tricular aneurysm (which can lead to
CHF, dysrhythmias, and embolism)
Inferior MU
Right coro
AV blocks (which can result in bradycarinferior left
nary (RCA)
dia) and papillary muscle dysfunction
venrricle
(which can result in valvular insufficiency and eventually CHF)
Anterolateral
Lefr anterior
Brady or rachyarrhythmias, acute ventric
Mllantero·
descending
ular sepral defecr
lateral left
(LAD), cirventricle
cumnex
Anrerosepral
LAD
Brady or tachyarrhythmias, ventricular
Mllsepral
aneurysm
regionberween left
and right
ventricles
Posterior Mll
RCA, circum
Bradycardia, heart blocks
posterior
flex
heart
Right venerieu
RCA
Right ventricular failure (can lead to left
lar MI
ventricular failure and therefore cardiogenic shock), heart blocks, hepacomegaly, peripheral edema
Transmural M l
Any artery
Full wall thickness MJ, as above
(Q-wave MI)
Subendocar
Any artery
Partial wall thickness Ml, as above,
dial MI
pocencial to extend to transmural MJ
(non-Qwave MI)
AV = atrioventricular; CHF = congestive heart failure; LAD = left amerior descending;
RCA = righr coronary anery.
Source: Data from SL Woods, ES Sivarajian-Froelicher. S Underhill-Moner (cds). Cardiac Nursing (4th ed). Philadelphia: Lippincon. 2000.
....
N
} hUmu wilh ST EkVJlion � � >-
l
ikely 10 !We ill with . Q ....... y.e Ml
They
g
ue abo (:OIl$ickm;l for
TlvomboIytic Thc:npy Of
'"
RevascularbauOQ procedures while in
I'
"dR.
i::
Ru1e In VlI. Rule
OutMI
J:
Delefmined by
�
Biochemical
"
M.mn
�
g
'"
IfpaDmIIlal:
If palienI bal lIO
o
If patient bas:
,.
Ifpatierlllw:
.........,. .....
compIicatiol'lJ and;
RCCllnull iJc:hcnua
�
",""", £CO
PAP>20mmHO
HoWoMI
CHF
J:
No Rest
S3 GoIIop
No bcbernic pWI
-<
"""M
Hypocensloa
H",....,....
SIIbIe Rhythm
�
""",.......
No Noaurnal
"""""' Sf aw.g.,
NoCHP
�
"""M
•
Heart block
""""'"
r
No Heart Block
May be considefeld:
Prior MI
HcmodyrwuicaUy
HiJh RiKICompIica&cdlUnst.ble
i
May be oonsid0=4:
......
lDw Riu I Stable
"'-y be oonsidered:
MI)'bc�:
�
Hip Rw - f\st1hcr Medical
Low RisklSUibIe
�
Wort-Up
�
Medical I SUtJical Tn:atmcnt
will dqIcDd on compUcabon.
Out oICCU 24.36
OiagnGAies will likely
Mly UI:IdI::r:to
HOIU1 af\c:r 1Idmiuion.
incNde. calheterizarion.
NoniJ!va5I."
Treatma'li ml)' Include IOIDI:;
StralTm
1f$tl,)'II uat»e and
or
� MD IDII)'
farm of�wioo.
C......,
�dlc:l4-4
I..mJIb of nay iI variabk.
Anmogaphy
CABO;
"""' _ ..
Ulu&lly
Uncomplicakd
OUI.,.rimt manqcmml
Dl5Chuged
-
III 1·2
die 4-7 days
Horpil&lization
0.,.
IOdacftuerisJr:
and atabilix
for-Klirit)'


CARDIAC SYSTEM
43
Clinical Tip
• (ST) depression, on a patient's ECG, of approximately
1-2 mm is generally indicative of ischemia.
• ST elevation is generally indicative of myocardial injury
or infarction.
Rhythm and Conduction Distl/ybance
Rhythm and conduction disturbances can range from minor alterations with no hemodynamic effects to life-threatening episodes with rapid hemodynamic compromise.·,s,7 Refer to Chapter
Appendix I -A for a description of atrial, ventricular, and junctional rhythms and AV blocks. Refer also to Chapter Appendix 1-8
for examples of common rhythm disturbances. Physical therapists
need to be able to identify abnormalities in the ECG to determine
patient tolerance to activity. In particular, physical therapists
should understand progressions of common ECG abnormalities so
they can identify, early on, when the patient is not tolerating an
intervention. (Refer to the Physical Therapy Intervention section
for the ECG discussion.)
.... Figure 1-9. Possible clinical course of patients admitted with chest pain.
(CABC = corollary artery bypass graft; CHF = cOl1gest;ve heart failure; CCU
= coronary care unit; die :: discharge; ECC :: electrocardiogramj h/o :: history
0(; MI :: myocardial infarctio1l; PAP = pulmonary arterial presmre; PTCA =
percutaneous translumjllal coronary angjoplasty; ST Elevatjon = electrocardiogram that shows elevatioll of the ST segment.) (Data from American College of Cardio/ogy/Americall Heart Associatioll. 1999 Update: ACCIAHA guidelines for the manageme11t of patiellls with acute myocardial infarction:
executive summary and recommendations. Circulation 1 999; 1 00: 1 016-1 030;
American College of Cardiology/American Heart Association. ACCIAHA
guidelines for the management of patients with acute myocardial infarction. J
Am Coli Cardiol 1 996;28:1328-1428; alld American College of Cardio/ogy/
American Heart Association. A CCiA HA guidelines for the management of
patients with ltltstable angina and Ilon-ST segment elevation myocardial
infarctioll. J Alii Coli CardioI 2000;36:971-1 048.)
