i bc27f85be50b71b1 (76 page)
Read i bc27f85be50b71b1 Online
Authors: Unknown
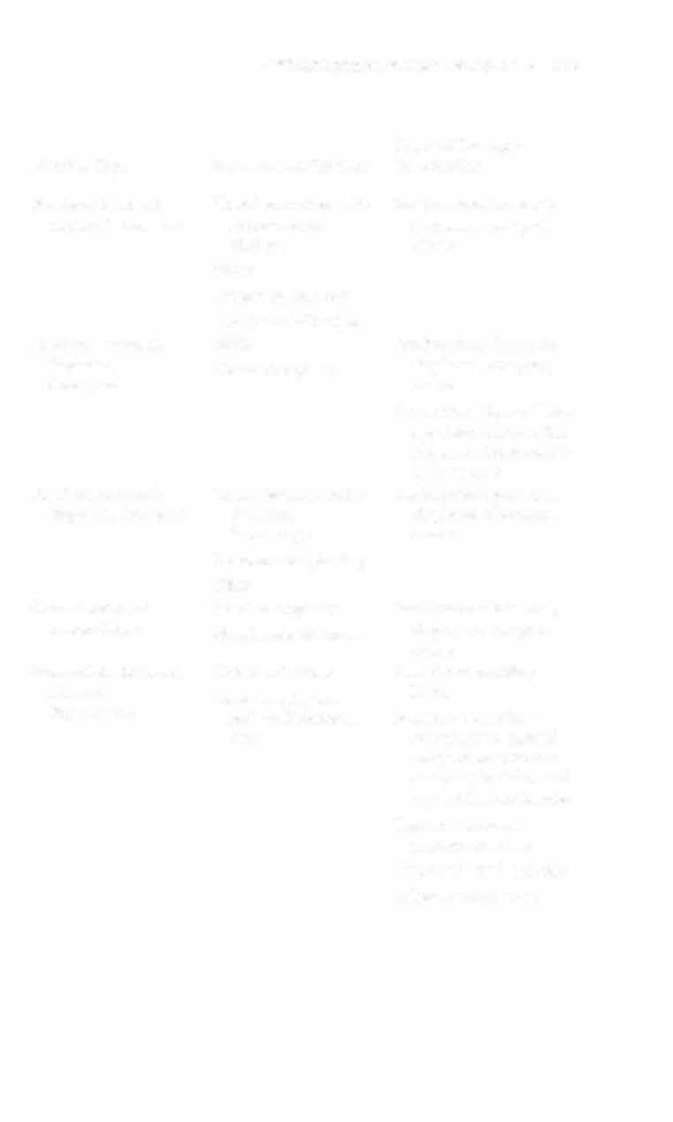
exercise
Edema management
Forefoot; moderate or
ORJF
Sec Forefoot; minimally
severe displacement, Percutaneous pinning
displaced, above
with fragmentation
or angularion
SLC
Forefoot; open
See Calcaneal;
See Forefoot; minimally
open, above
displaced, above
ORIF
NWB = non weight bearing; ORIF = open-reduction internal fixatioll; PWB = partial
weight bearing; ROM = range of motion; SLC = short leg cast; WBAT = weight bearing
as tolerated.
'"For calcaneal fractures, cast application may not be in the neutral ankle position to
protect the fracture site from strong ankle muscle contractions.
Source: Data from JD Heckman. Fractures and Dislocations of the Foot. In CA Rockwood, DP Green, RW Bucholz, JD Heckman (cds). Rockwood and Green's Fractures in Adults (4th cd). Philadelphia: Lippincon-Raven, 1996.

252 AClITE CARE HANDBOOK FOR PHYSICAL TIIERAPISTS
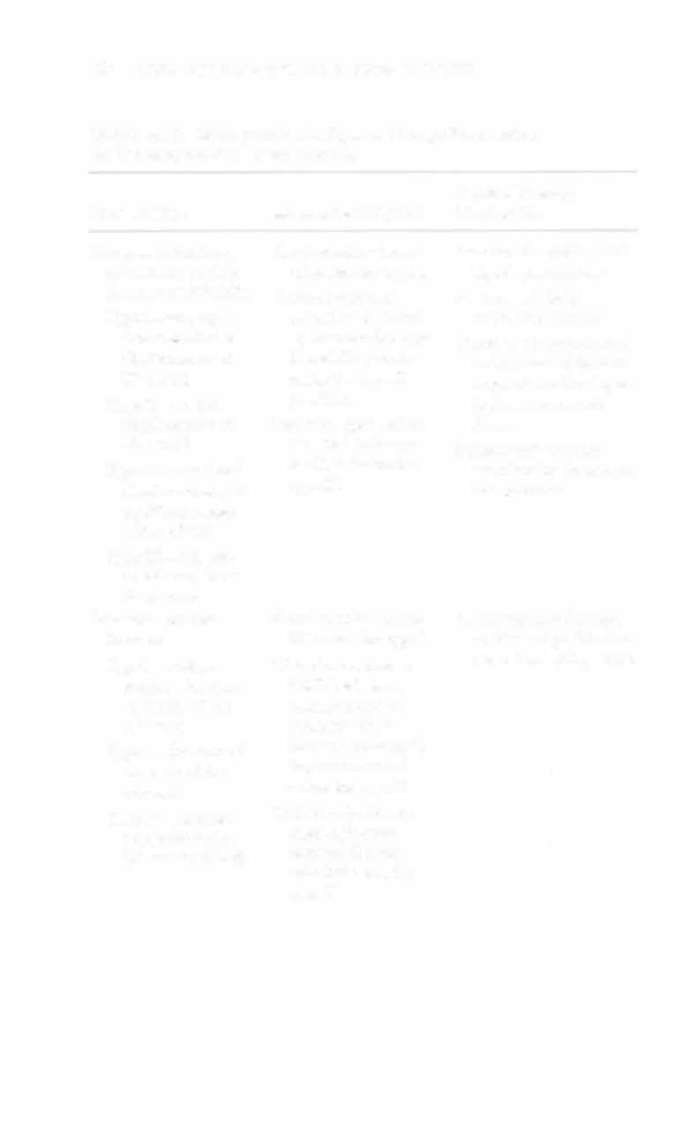
Table 3-A.12. Management and Physical Therapy Imervention
for Common Cervical Spine Fractures
Physical Therapy
Fracture Type
Management Options
Intervention
Hangman's fracture,
Cervical collar immo
Functional mobility with
or bilateral pedicle
bilization for type I
logroll precautions
fracrure of axis IC I ) Cervical traction!
Posture and body
Type I-no angula-
reduction followed
mechanics training
tion and <3 mm
by halo vest for type
Therapeutic exercise and
displacement of
II and ItA (cervical
active-assisted/passive
C2 on C3
collar for type II
range of motion depcn
Type 11->3 mm
possible)
dent on neurologic
displacement of
Posterior open reduc
IIlJury
C2 on C3
tion and halo vest
Balance and scapular
Type !lA-minimal
or CT-3 fusion for
exercises for the patient
displacement and
type 11\
in a halo vest
significant angulation of C2
Type III-full unior bilateral facet
dislocation
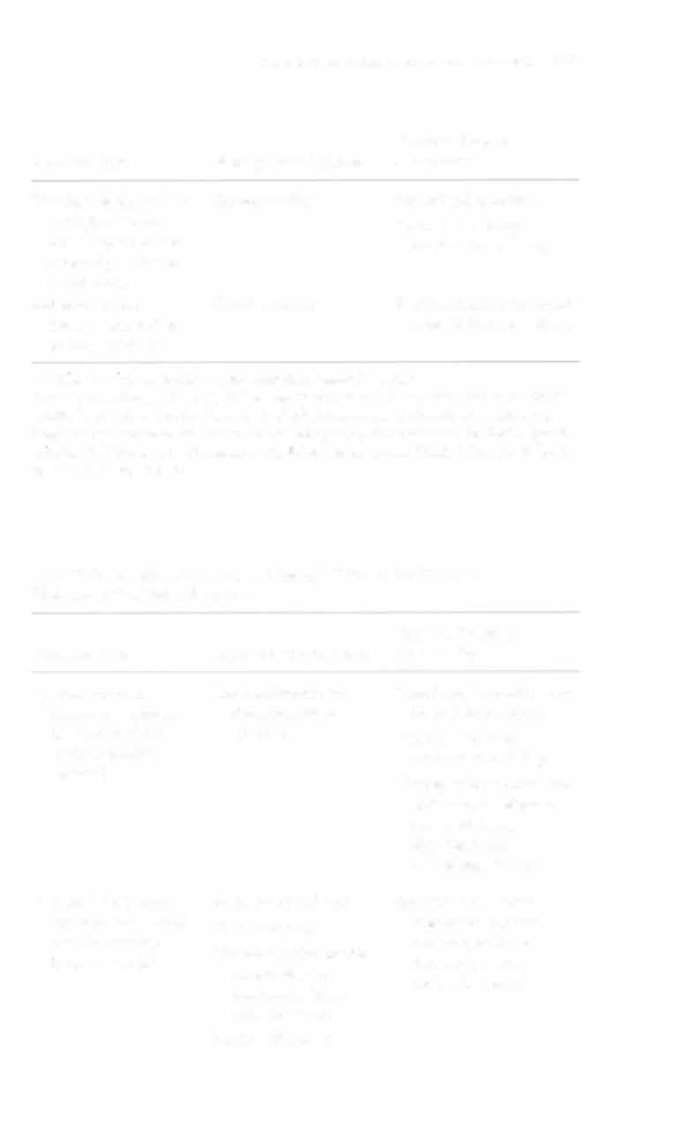
Odontoid process
Cervical collar immo
See Hangman's fracture,
fracture
bilization for type I
or bilateral pedicle frac
Type l-
Closed reduction or
tUfe of axis (GI), above
avulsion fracture
ORIF with halo
of the tip of the
vest, amerior or
odontoid
posterior C 1-2
T ypc II-fracture of
fusion::!: bone graftthe neck of the
ing with cervical
odontoid
collar for type II
Type 1I1-fracture
Closed reduction or
extending ro the
open-reduction
C2 vertebral body
inrernal fixation
with halo vest for
type 11\

MUSCULOSKELt:.iAL SYSTEM APPENDlX 3�A
253
Physical Therapy
Fracture Type
Management Oprions
Intervention
Vertebral body (stable
Cervical collar
Functional mobility
wedge) fracture-
Posture and body
bony impacrion and
mechanics training
concavity of the ver-
tebral body
Spinous process
Cervical collar
Sec Vertebral body (stable
(stable, isolated) or
wedge) fracture, above
laminal fracture
j: = With or wlthom; ORIF = open-reduction internal fixarion.
Sources: Data from RC Sasso, TM Reilly. Odontoid and Hangman's Fractures. Orthopaedic Knowledge Update: Trauma (2nd ed). Rosemont, IL: American Academy of Orthopaedic Surgeons, 2000; and RS Hockberger, KJ Kirshenbaum, PE Doris. Spinal
Injuries. In P Rosen (cd), Emergency Medicine Conceprs and Clinical Practice (4th ed).
St. Louis: Mosby. 1998.
Table 3-A.13. Management and Physical Therapy for Common
Thoracolumbar Spine Fractures
Physical Therapy
Fracture Type
Management Options
Intervention
Spinous process,
Cervicothoracic or
Functional mobility with
rransverse process,
thoracolumbar
logroll precaurions
laminar, or facet
orrhosis
PoSture and body
fracture (stable,
mechanics training
isolated)
Therapeutic exercise and
active-assisted/passive
range of morion
dependent on
neurologic injury
Vertebral body com
Shorr-term bed rest
See Spinous process,
pression (impacted
Verrebroplasty
transverse process,
anterior wedge)
laminar, or facet
Thoracolumbar or rho-
fracture--srable
fracture (stable,
racolumbosacral
isolated), above
orthosis or hyperextension brace
Fusion (if severe)
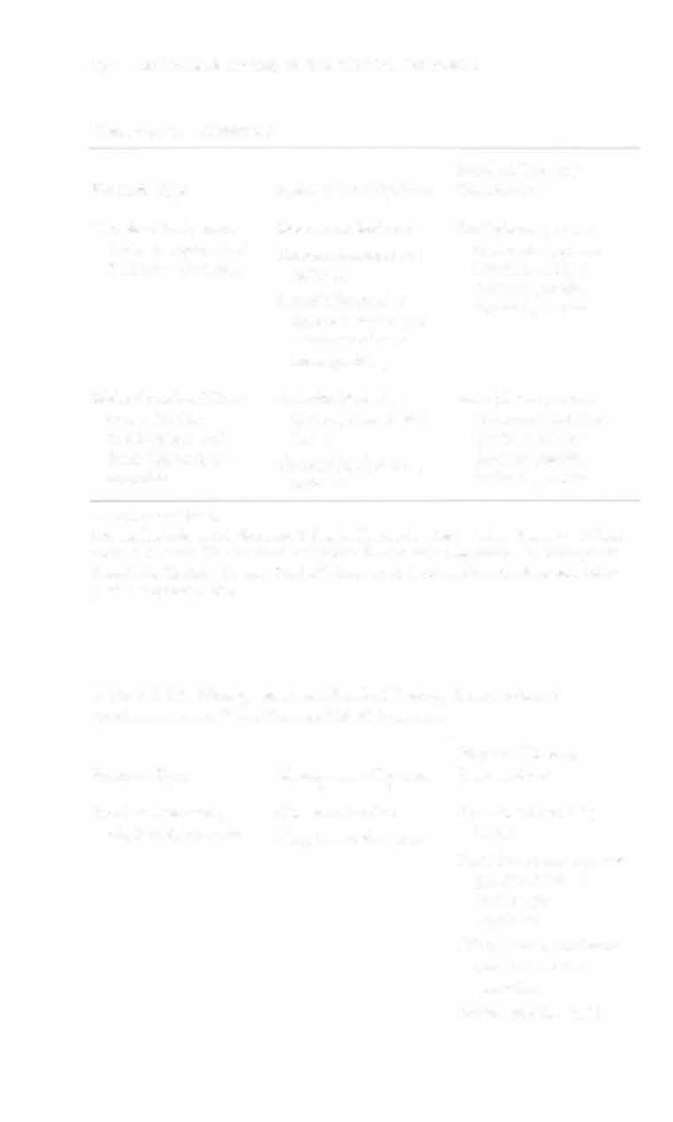


254 AClJfE CARE HANDBOOK FOR PHYSICAL THERAPISTS
Table 3 - A.13. Continued
Physical Therapy
F ractu re Type
Management Options
Intervention
Vertebral body burst
Short-term bed rest
See Spinous process,
(axial compression)
Thoracolumbosacral
transverse process,
fracture-unstable
orthosis
laminar, or facer
fracrure (stable,
Anterior/posterior
isolated), above
decompression and
reconstruction :t:
bone grafting
Multidirectional frac
Anterior/posterior
See Spinous process,
ture with disc
decompression and
transverse process,
involvement and
fusion
laminar, or facet
facet dislocarion
Thoracolumbosacral
fracture (stable,
unstable
orthosis
isolated), above
:!: = with or without.
Source: Data from AR Vaccaro, K Singh. Thoracolumbar Injuries: Nonsurgical Treatment. DC Kwok. Thoracolumbar Injuries: The Posterior Approach. In Orthopaedic Knowledge Update: Trauma (2nd ed). Rosemont, IL: American Academy of Orthopaedic Surgeons, 2000.
Table 3 - A.t4. Management and Physical Therapy Intervention of
Proximal Humeral· and Humeral Shaft Fractures
Physical Therapy
F racture Type
Management Options
Intervention
Proximal humeral;
Closed reduction
Functional mobility
displaced, one-part
Sling immobilization
NWB
Pendulum exercises and
passive range of
motion per
physician
Elbow, wrist, and hand
range-of-morion
exercises
Edema management