i bc27f85be50b71b1 (87 page)
Read i bc27f85be50b71b1 Online
Authors: Unknown


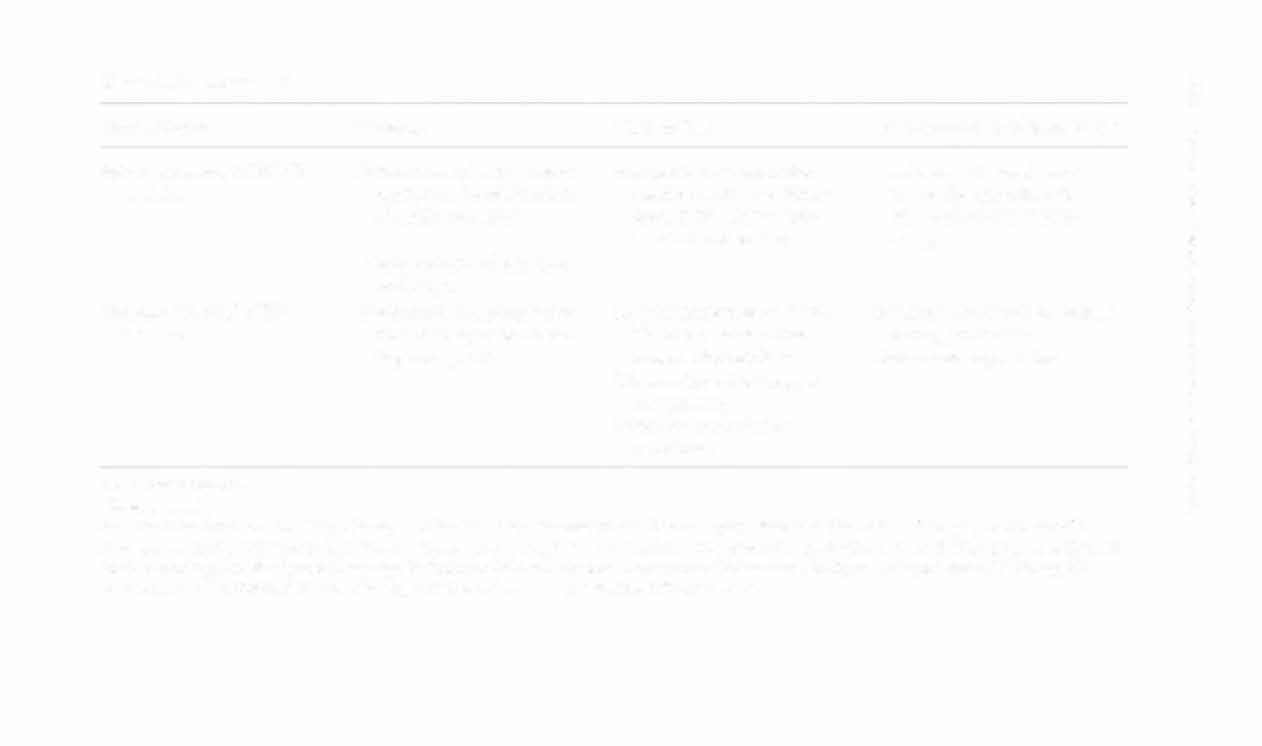
Oculomotor (CN lII)bmd.
Upward, inward, Jnd mfero-
eNs III, IV, and VI are
Ophthalmoplegia with eye
hrdm
medial cyc movemcllf
tcsted rogcther.
dcviation downward and
outward
Eyelid eleva non
Pupd reaction [Q light: Shme
ProSIS
a flashlight inro one eye
and observe bilateral
pupil reaction.
Pupil (onstricflon
Gaze: Hold oblect (e.g., pcn)
Loss of ipsilateral pupillary
Visual focuslllg
at arm's length from the
light and accommodation
patient, and hold the
refle"(es
patient'S head steady, Ask
the patient to follow the
object with a full honzon·
tal, vertical, and diagonal
gaze.
Trochlear (eN N)/I/I/dbra/ll
Inferolateral e}'c movement
See Oculomotor (eN III),
Diplopia
and proprioception
above.
Head nit to unaffected side
Weakncss in depression of
ipsilateral adducted eye
Trigeminal (eN V)/pOIIS
Sensation of face
Conduct rouch, pam, and
Loss of facial sensation
z
'"
temperature sensory test·
"
i§
ing over the patiem's face.
5i
Mastication
Observe for deviation of
Ipsilateral deviation of opened
�
-<
Jaw.
Jaw
�
;:
...
00
'"




Table 4-13. Continued
N
'"
0
Nerve/Origin
Purpose
How to Test
SignS/Symptoms of Impairment
>
()
Cornea I reflex
Wisp of cotton on [he
Loss of ipsilateral corneal
�
patient's cornea.
reflex
()
>
'"
Jaw jerk""
Palpate masseter as the
'"
patient clamps his or her
J:
>
z
jaw.
"
Abducens (eN VI)lpons
Lateral eye movement and
See Oculomotor (eN III),
Diplopia
15
0
proprioception
above.
Convergent strabismus
'"
Ipsilateral abductor paralysis
d
'"
Facial (eN VII)lpons
Taste (anterior rwo-thirds of
Ask the patient to smiJe,
Paralysis of ipsilateral upper
�
�
tongue)
wrinkle brow, purse lips,
and lower facial muscles, loss
�
and close eyes tightly.
of lacrimation, dry mouTh,
n
>
r
Facial expression
Inspect closely for
loss of taste on ipsilateral
:i
symmetry.
two-thirds of tongue.
'"
'"
Autonomic innervation of
>
�
lacrimal and salivary
�
glands
VeStibulocochlear (eN VIII)I Vestibular branch: sense of
Oculocephalic reAex (Doll's
Vertigo, nystagmus,
pons
equilibrium
eyes): Rotate the patient's
disequilibrium, neural
head and watch for eye
deafness
movement.
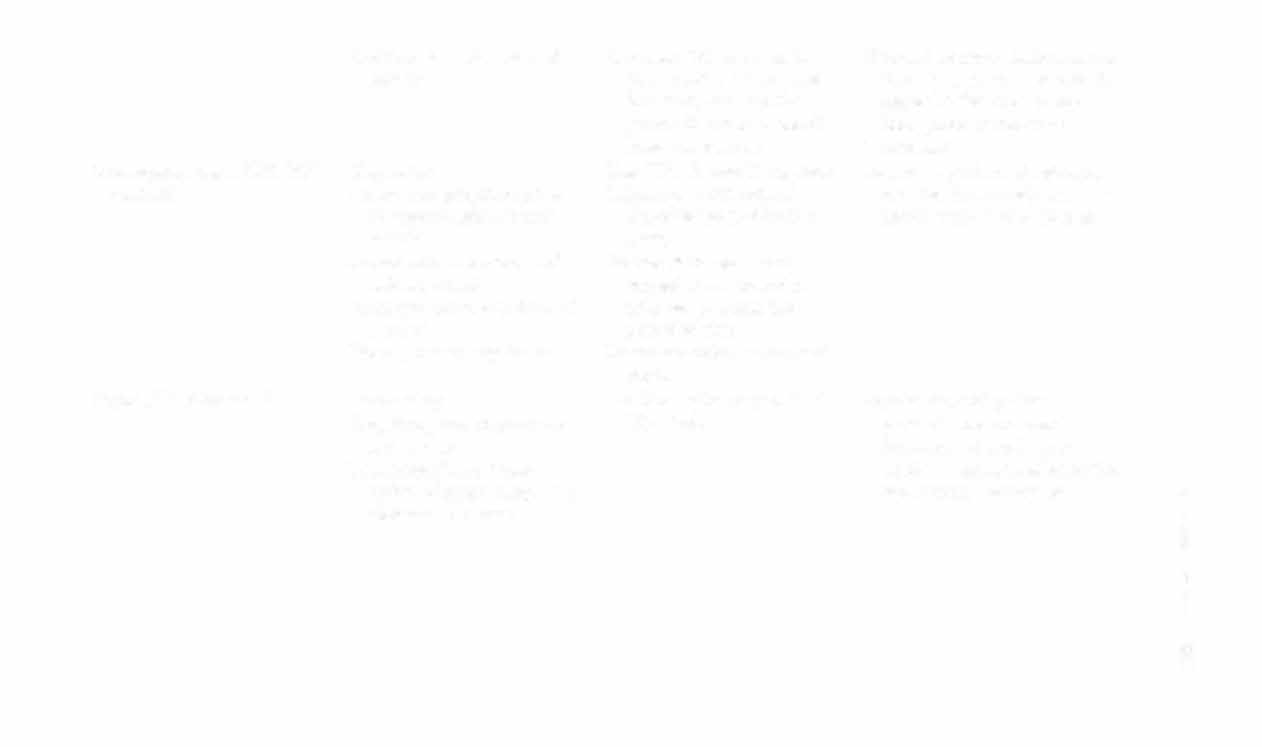
Cochlear branch: sense of
Cochlear: Vibrate a tuni,ng
(Normal oculocephalic reflex is
hearing
fork, place it on the mid
that the eyes will move in the
forehead, and ask the
opposite direction of the
patient if sound is heard
head prior [0 return ro
louder in one ear.
midline)
Glossopharyngeal (eN [Xli
Gag reflex
Test CNs IX and X coger her.
Loss of gag reflex, dysphagia,
medulla
Motor and proprioception
Induce gag with tongue
dry mouth, loss of taste ipsiof superior pharyngeal
depressor (one side at a
lateral one-third of tongue
muscle
time),
Autonomic innervation of
Patient phonates a prosalivary gland
longed vowel sound or
Taste (posterior one-third of
talks for an extended
tongue)
period of rime.
Blood pressure regulation
Listen for voice quality and
pitch.
Vagus (eN X)/medulla
Swallowing
See Glossopharyngeal (eN
Dysphagia, soft palate
Proprioception of pharynx
IX), above.
paralysis, contralateral
and larynx
deviation of uvula, ipsi
Parasympathetic innerlateral anesthesia of pharynx
vation of hearr, lungs, and
and larynx, hoarseness
abdominal viscera
�
(§
c
�
�
-<
�
N
'D
�