i bc27f85be50b71b1 (24 page)
Read i bc27f85be50b71b1 Online
Authors: Unknown
for a patient or may result in an unstable physiologic response.
Unstable responses provide some indication that the patient is nOt able
to meet physiologic demands owing to the pathologic process for the
level of work that the patient is performing. In this siruation, the physical
therapist needs to consider the patient'S response to other activities and
determine whether these activities create a stable response. If it is stable,
can the patient function independently doing that level of work?
For example, some patients may be stable walking 10 ft to the
bathroom at one time, yet this activity may require maximal exertion
for the patient and therefore should be considered too much for the
patient to continue to do independently throughout the day.
If the patient'S response is nOt stable, then the therapist should try to
discern why it is not stable, along with finding out if anything can be
CARDIAC SYSTEM 63
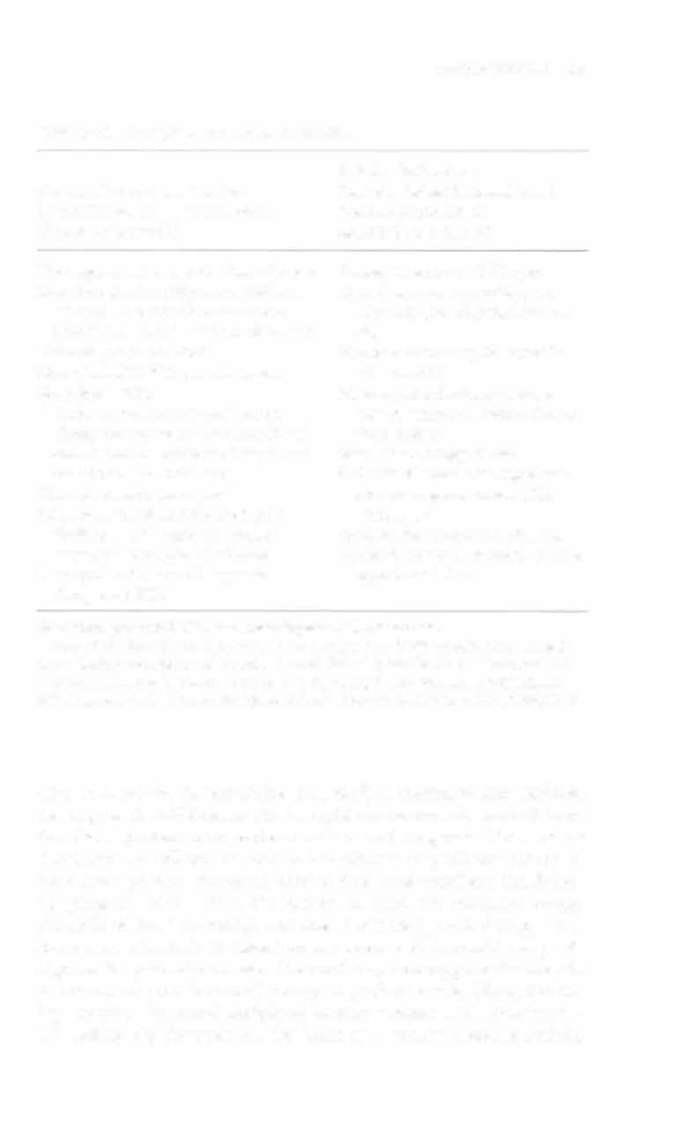
Table 1-2 1 . Indications of Patient Instability
Relative Indications
Absolute Indications That the
That the Patient Is Unstable and
Patient Is Unstable and Treatment
Treatment Should Be
Should Be Withheld
Modified or Withheld
Decompensated congestive heart failure Resting heart rate > 100 bpm
Second-degree heart block coupled with
Hypertensive resting BP (syscolic
premature ventricular contractions
> 160 mm Hg, diascolic >90 mm
(PVCS) of ventricular tachycardia at rcst
Hg)
Third-degree heart block
Hypotensive resting BP (systolic
More than 1 0 pves per min at rest
<80 mm Hg)
Multifocal PVCs
Myocardial infarction or exten
Unstable angina pectoris with recent
sion of infarction within the prechanges in symptoms (less than 24 hrs)
vious 2 days
and electrocardiographic changes asso
Ventricular eccopy at rest
ciated with ischemia/injury
Atrial fibrillation with rapid ven
Dissecting aorric aneurysm
tricular response at rest (HR
New onset (less than 24 hrs) of atrial
> 100 bpm)
fibrillation with rapid ventricular
Uncontrolled metabolic diseases
response at rest (HR > 100 bpm)
Psychosis or other unstable psycho
Chest pain with new ST segment
logical condition
changes on ECG
BP = blood pressure; ECG = electrocardiogram; HR = heart rate.
Sources: Data from LP Cahalin. Heart failure. Phys Ther 1 996;76:520; MH Ellestad.
Stress Testing: Principles and Practice (4th cd) Philadelphia: FA Davis, 1 996; and NK
Wegener. Rehabilitation of the Patient with Coronary Heart Disease. In RC Schlant,
RW Alexander (cds), Hurst's the Heart (8th cd). New York: McGraw-Hili, 1994;1 227.
done to make the patient stable (i.e., medical treatment may stabilize
this response). Additionally, the therapist should find the level of function that a patient could perform with a stable response. However, at times, patients will not be able to be stabilized to perform activity. In
these cases, physical therapists need to determine whether a conditioning program would allow the patient to meer the necessary energy demands without becoming unstable. Proceeding with therapy at a
lower level of activity is based on the premise that conditioning will
improve the patient'S response. The cardiac system suppOrts the body in
its attempt to provide enough energy to perform work. Often, becoming stronger-increased peripheral muscle strength and endurancewill reduce the demands on the heart at a certain absolute activity