i bc27f85be50b71b1 (22 page)
Read i bc27f85be50b71b1 Online
Authors: Unknown
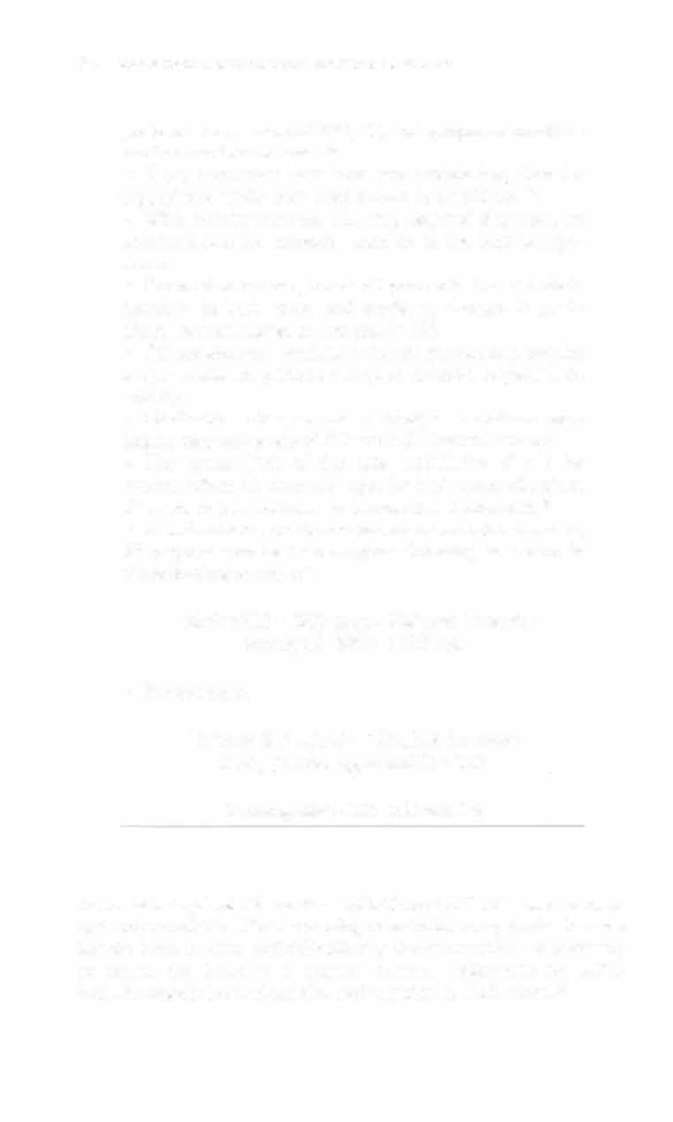
Modulation
Function
0 = None
N = None
0 = None
0 = None
0 = None
A = Arrium
A = Atrium
I = Inhibited
S = Simple
P = Pacing
programmable
V = Ventricle
V Ventricle
T = Triggered
M = Multi-
S Shock
=
=
programmable
D Dual
D = Dual
D = Dual
C = Communicating
D = Dual
=
R = Rate modulacion
Dual = atrium and ventricle can be sensed and/or paced independently; Inhibited = pending stimulus is inhibited when a sponraneous stimulation is detected; Triggered = detection of stimulus produces an immediate stimulus in the same chamber; Simple programmable = program either rate or output; Mulriprogrammablc = can be programmed more extensively; Communicating = has telemetry capabilicies; Rate modulation = can adjust ute automatically based on one or more physiologic variables.
Source: Adapted from AD Bernstein, AJ Camm, RD Fletcher, er al. The NASPElBPEG generic pacemaker code for anribradyarrhythmia and adaptive pacing and anritachyarrhythmia devices. PACE 1987;10:795.
Q
:;
� � -< �
'"
'"


56
ACUTE CARE HANDBOOK FOR PHYSICAL THERAI)ISTS
preferred. Assessment of RPE, BP, and symptoms should be
used ro moniror rolerance.48
•
If the pacemaker does have rate modulation, then the
type of rate modulation used should be considered":
• With activity sensors, HR may respond sluggishly to
activities that are smooth-such as on the bicycle ergometer.
•
For motion sensors, treadmill protocols should include
increases in both speed and grade, as changes in grade
alone may nOt trigger an increase in HR.
• QT sensors and ventilarory driven sensors may require
longer warm-up petiods owing to delayed responses to
activity.
• Medication changes and electrolyte imbalance may
impact responsiveness of HR with QT interval sensors.
• The upper limit of the rate modulation should be
known. When HR is at the upper limit of rate modulation,
BP needs ro be monitored ro be sure it is maintained.48
•
In individuals who do not have rate modulated pacers,
BP response can be used ro gauge intensity, as shown 111
the following equation" :
Training SBP = (SBP max - SBP rest) (intensity
usually 60-80%) + SBP rest
•
For example,
Training SBP = ( 1 80 - 120)(10.6 for lower
limit] [0.8 for upper limitJ) + 1 20
Training SBP = 1 56-1 68 mOl Hg
A utomatic implalltable cardiac defibrillator (AI CD) is used to manage uncontrollable, life-threatening ventricular arrhythmias by sensing the heart rhythm and defibrillating the myocardium as necessary to return the heart to a normal rhythm. Indications for AICD
include ventricular tachycardia and ventricular fibrillation. II


CARDIAC SYSTEM
57
Value Repiacemell(
Valve replacement is an acceptable method for treatment of valvular
disease. Patients with mitral and aortic stenosis, regurgitation, or
both are the primary candidates for this surgery. Like the CABG, a
median sternotomy is the route of access to the heart. Common valve
replacements include mitral valve replacements and aortic valve
replacements. Prosthetic valves can be classified as mechanical (bileaflet and tilting disc valves are commonly used) as well as biological valves (derived from cadavers, porcine, or bovine tissue),
Mechanical valves are preferred if the patient is younger than 65
years and is already on anticoagulation therapy (commonly due to history of atrial fibrillation or embolic cerebral vascular accident). The benefit of mechanical valves is their durability and long life.'2 Mechanical valves also tend to be thrombogenic and, therefore, require lifelong adherence to anticoagulation. For this reason, they may be contraindicated in patients who have a history of previous bleedingrelated problems, wish to become pregnant, or have a history of poor medication compliance. These patients may benefit from biological
valves since there is no need for anticoagulation therapy. Biological
valves may also be preferred in patients older than 65 years of age.t2
Postoperative procedures and recovery from mitral valve replacement
and aortic valve replacement surgeries are very similar to CABG,ll
Dyllamic Cardiomyoplasty
Dynamic cardiomyoplasry uses the latissimus dorsi muscle to provide
a muscular assist to the left ventricle during systole for patients with
dilated cardiomyopathies." The latissimus dorsi is detached distally,
moved forward, and wrapped around the left ventricle. The latissimus
dorsi is mechanically paced to contract with cardiac contraction. It
takes approximately 12 weeks for transformation of the latissimus
dorsi's contractile structure to correspond to cardiac requirements,
and patients may not receive benefit for 2-3 months '· Moving the
latissimus dorsi may restrict the thorax and result in atelectasis, which
needs to be addressed in postoperative physical therapy intervention.
This procedure is reserved for patients with end-stage heart failure
who have limited treatment options.4• In light of the marginal benefits
and high postoperative mortality rates, the cominued use of dynamic
cardiomyoplasty has recently been questioned "
58
ACUTE CARE HANDBOOK FOR PHYSICAL ll-IERAI}ISTS
Partial Left Ventriculectomy (Batista Procedure)
The Batista procedure reduces the volume of the left ventricular
chamber radius through surgical resection of a portion of the myocardium.46 This in turn decreases wall tension and improves diastolic filling. To reduce the negative effects of mitral regurgitation, the mitral valve is repaired or replaced during the surgery. The initial study of patients receiving this procedure included individuals with New York Heart Association Class IV heart failure. Patients
are generally discharged in 7 to 10 days, and low-level activity can
begin as soon as the patient is hemodynamically stable, although
vigorous exercise is deferred for 6 to 8 weeks postoperatively.46
Like other relatively new, experimentally available procedures, this
procedure has generally been reserved for patients with end-stage
heart failure who have limited treatment options. The procedure
requires a sternotomy and the concomitant sternal precautions, as
discussed after CABG.
Cardiac Transplantation
Cardiac transplantation is an acceptable intervention for rhe rreatment of end-stage heart disease. A growing number of facilities are performing heart transplantation, and a greater number of physical therapists are involved in the rehabilitation of pre- and POSttransplant recipients. Physical therapy intervention is vital for the success of heart transplantation, as recipienrs have often survived a