i bc27f85be50b71b1 (93 page)
Read i bc27f85be50b71b1 Online
Authors: Unknown
cytokines and a disruption of the blood-brain barrier, which causes
the development of vasogenic (extracellular) brain edema; impaired
cerebral autoregulation and ischemia in the setting of hypoxia and
hypotension; tissue acidosis and an influx of electrolytes, which
causes cytotoxic (intracellular) brain edema; and the loss of neurons,
glial cells, and presynaptic terminals from neurochemical and oxygen
free radical reactions.17.18
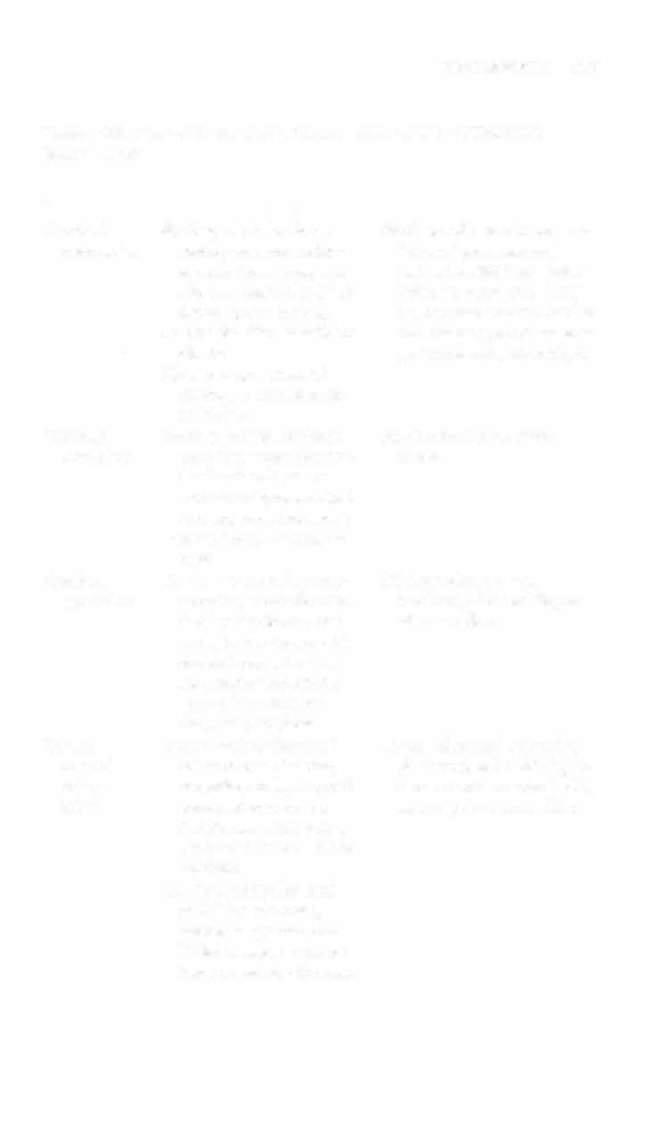
Table 4- 1 8 defines the most common types of TBI and describes
the clinical findings. The management of these conditions is discussed
later in General Management and in Table 4-2 1 .
Spil/al Cord II/jury
Spinal cord injury (SCI) and the resultant para- or quadriplegia are
typically due to trauma or, less frequently, impingement of the spinal
cord from abscess, ankylosing spondylitis, or tumor. Primary SCI, the
direct trauma at the time of injury, can be described according to
location or mechanism of injury29:
1 .
Location. SCI may involve the cervical, thoracic, or lum-
bar spines.
2.
Mechanism of injury. SCI may result from blunt or penetrat-
ing injuries. Blunt forces include ( I ) forward hyperOexion, causing the
discontinuity of the posterior spinal ligamenrs. disc herniation, and

NERVOUS SYSTEM
307
Table 4-18. Clinical Findings and General Management of Traumatic
Brain Injuries
Injury
Definition
Clinical Findings
Cerebral
Shaking of the brain sec-
Brief loss of consciousness or
concussion
ondary (Q acceleration
"dazed" presentation,
deceleration forces, usuheadache, dizziness, irritaally as a result of a fall or
bility, inappropriate laughduring sports activity.
ter, decreased concentration
Can be classified as mild or
and memory, rerro- or anreclassic.
grade amnesia, altered gait
Signs and symptoms of
cerebral concussion are
reversible.
Cerebral
Bruise (small hemorrhage)
See Cerebral concussion,
contusion
secondary to accelerationabove
deceleration forces or
beneath a depressed skull
fracture. most commonly
in the frontal or temporal
areas.
Cerebral
Tear of the cortical surface
SIS dependent on area
laceration
secondary to accelerationinvolved, JCr, and degree
deceleration forces, comof mass effect
monly in occurrence with
cerebral contusion over
the anterior and middle
fossa where [here are
sharp bony surfaces.
Diffuse
Occurs with widespread
Coma, abnormal posturing
axonal
white matter shearing
(if severe), other SIS depeninjury
secondary to high-speed
dent on area involved, ICP,
IDAI)
accelerarion-decelera -
and degree or mass effect
tion forces, usually as a
result of a motor vehicle
accident.
Can be classified as mild
16-24 hrs of coma),
moderare (greater than
24 hrs coma), or severe
(days ro weeks of coma).

308
AClITE CARE HANDBOOK I:OR PHYSICAL THERAPISTS
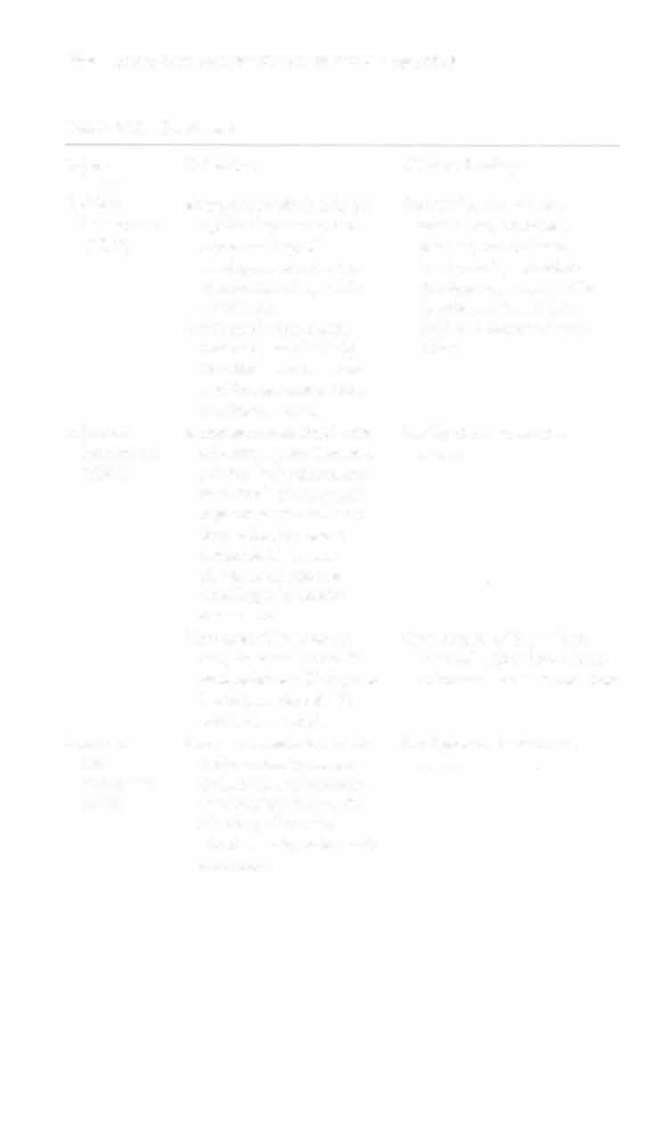
Table 4-18. Continued
Injury
Definition
Clinical Findings
Epidural
Blood accumulation in the
Headache, altered COIlhematoma
epidural space secondsciousness, abnormal
(EDH)
ary ro tearing of
posture, contralateral
meningeal arteries that
hemiparesis, and other
compresses deep brain
SIS dependent on specific
structures.
location of rhe lesion,
Associated with cranial
ICP, and degree of mass
fractures, particularly
effect
the thin temporal bone
and frontal and middle
meningeal tears.
Subdural
Blood accumulation in the
See Epidural hemaroma,
hematoma
subdural space that comabove
(SDH)
presses brain structures
as a result of traumatic
rupture or tear of cerebral veins, increased
intracranial hemorrhage, or cominued
bleeding of a cerebral
contusion.
The onset of symptoms
Can present with a "lucid"
may be acute (up to 24
interval before loss of conhrs), subacme (2 days to
sciousness for a second time
3 wks), or chronic (3
wks to 3-4 mas).
Intracere
Blood accumulation in the
See Epidural hematoma,
bral
brain parenchyma secabove
hematoma
ondary to acceleration
(ICH)
deceleration forces, the
shearing of cortical
blood vessels, or beneath
a fracmre.
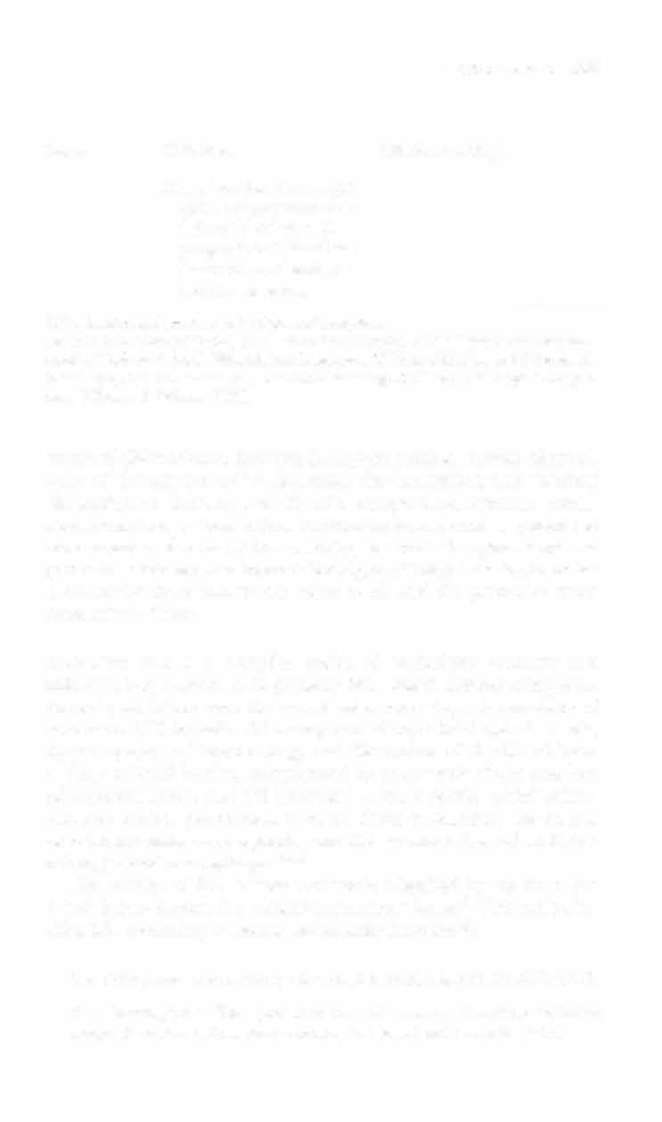


NERVOUS SYSTEM
309
Injury
Definirion
Clinical Findings
May also arise as a complicarion of hypertension or
delayed bleeding with
progression of blood into
the dural, arachnoid, or
ventricular spaces.
ICP = intracranial pressure, SIS = signs and symploms.
Sources: Data from JV Hickey (ed). The Clinical Practice of Neurological and Neurosurgical Nursing (4th ed). Philadelphia: Lippincon, 1997; and SA Mayer, LP Rowland.
Head Injury. In LJ> Rowland (ed). Merrirr's Neurology ( I Orh cd). Philadelphia: Lippincan, Williams & Wilkins, 2000.
vertebral dislocation or fracture; (2) hyperextension, causing discontinuity of the anrerior spinal ligaments, disc herniation, and vertebral dislocation or fracture; and (3) axial compression, rotation, contusion, laceration, or transection. Penetrating forces, such as gunshot or stab wounds, may be ( 1 ) low velocity, in which the spinal cord and
protective structures are injured directly, or (2) high velocity, in which
a concussive force injures the spinal cord, and the protective structures remain intact.
Seco/ldary SCI is a complex series of pathologic vascular and
innammatory responses to primary SCI, which further compound
the original injury over the course of several days. A summary of
secondary SCI includes ( 1 ) vasospasm of superficial spinal vessels,
intra parenchymal hemmorhage and disruption of the blood-brain
and spinal cord barrier, complicated by neurogenic shock and loss
of autoregulation, and (2) increased calcium levels, which stimulate frce radical production to cause further ischemia, the release of catecholamines and opioids, and the accumulation of activated
microglia and macrophages.29,3o
The severity of SCI is most commonly classified by the American