i bc27f85be50b71b1 (60 page)
Read i bc27f85be50b71b1 Online
Authors: Unknown
192
AClffE CARE HANDBOOK FOR PHYSICAL THERAPISTS
Figure 3-13. Bilateral total h;p arthroplasty.
components has the advantage of biological fixation, reducing the
incidence of aseptic loosellillg (the loosening caused by wear debris
from the components). With uncemented components, weight bearing
can be limited by surgeon protocol, but weight bearing should not be
discouraged.38 Weight bearing promotes bony ingrowth with the
uncemented prosthetic components by allowing physiologic strain in
the bone, thus increasing the activity of remodeling. With uncemented
THA, the emphasis for the patient should be the prevention of torque
or twisting on the operated leg while weight bearing.
The use of a cemented prosthesis (usually the femoral component)
is reserved for an individual with a decreased ability to regenerate
bone, such as a patient with osteopenia or osteoporosis.J9 A cemented
prosthesis allows fot full weight bearing early in the recovery phase.
A bipolar prosthesis consists of a metallic acetabular cup and polyethylene liner with a snap-fit socket placed over a femoral prosthesis, as shown in Figure 3_14.40 A bipolar prosthesis is a type of hip
arthroplasty used for revision when there is instability caused by
osseous or muscular insufficiency that makes a patient's hip morc
likely to dislocate.
Surgical approaches and movement precaurions for THA are presented in Table 3_64'.42 A good understanding of the surgical approach taken to expose the hip joint is necessary to determine
movement precautions that prevent dislocation postoperatively. In the
acute care setting, the risk of dislocation is significant because of the









.\tUSCULOSKEU:,IAL SYSTEM
193
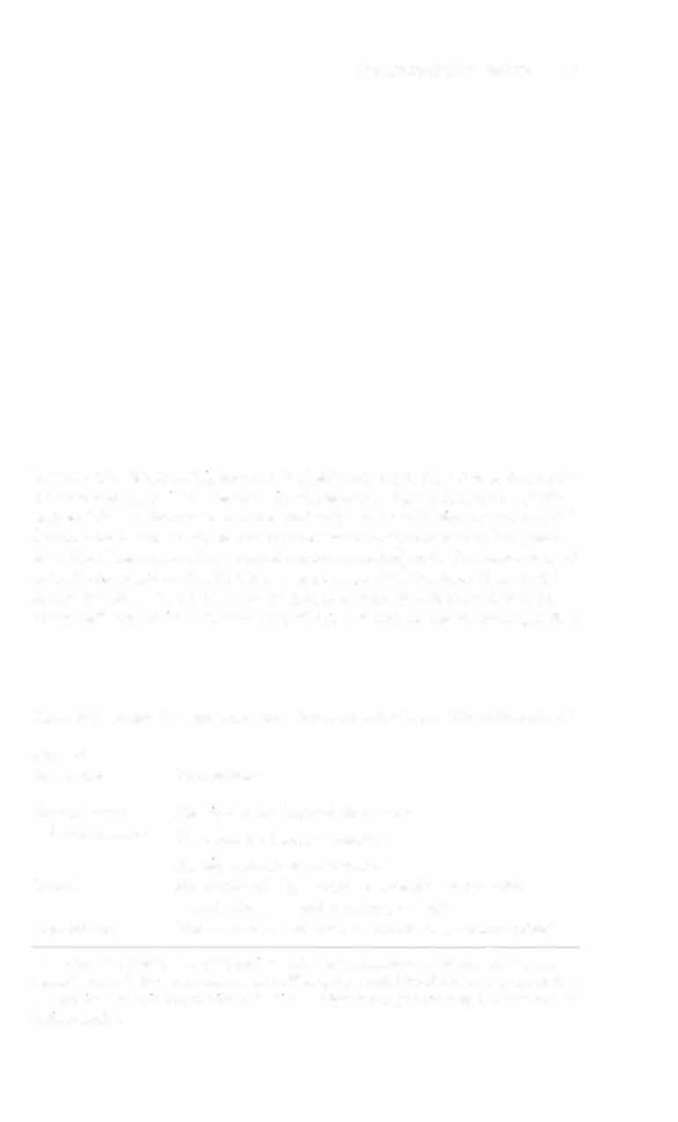
Figure 3-14. Mcuhfied bIpolar CliP. Polyetbylene CLIP IS placed over bead, and
the" the metal cup IS pressed over It. polyetbylene Imer is locked m metallic
cup, and bead is locked In socket of polyethylene liner. EntIre cup moves lvith
femoral head as olle lIlIIt, so cup canllot assume valglls or varus fixed positiol1. Metal bead ca" rotate HI plastIC socket m aXIS of neck. CliP mllst be used witb the femoral prostheSIS designed to fit properly mto plastic liner. (Wllh
permisS/oll (rom JIV Harkess. Arthroplasty o( Hip. In AH Crenshaw [edj,
Cmllpbd/'s OperatIve OrthopaedIcs, Vol. 1 [8th edj. St. LOllis: Mosby, 1998.)
Table 3-6. Surgical Approaches and Precaurions for Toral Hip Anhroplasry"
Surgical
Approach
Precnutions
Posterolateral
No hip flexion beyond 90 degrees
(most common)
No excessive internal rotation
No hip adduction past neutral
Lnteral
No combined hip flexion beyond 90 degrees with
ndduccion, internal rmation, or bmh
AnterolMeral
Hip extension and external rotation are to be avoided
·Hlp !ourgcry performcd in conJunction with a trochanteric ostcotomy (removal and
rc.machmcOi of the gre.1tcr trochanter) will require an additional movcment restriction
of no active abduction or pa!osive adduction. Weight bearing of the surgical limb may be
limned further.