Examination Medicine: A Guide to Physician Training (85 page)
Read Examination Medicine: A Guide to Physician Training Online
Authors: Nicholas J. Talley,Simon O’connor
Tags: #Medical, #Internal Medicine, #Diagnosis
ACTH = adrenocorticotrophic hormone; FSH = follicle-stimulating hormone; LH = luteinising hormone; TSH = thyroid-stimulating hormone.
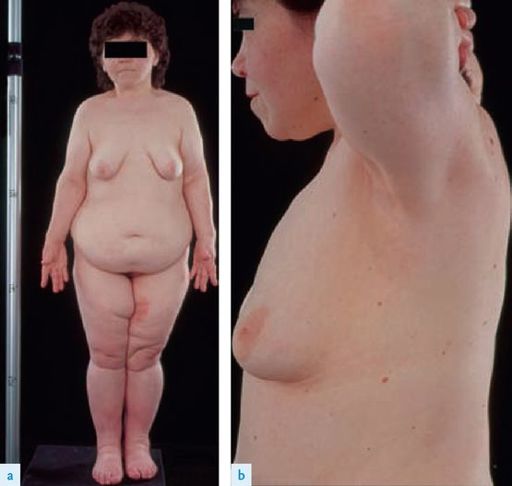
FIGURE 16.44
Panhypopituitarism. (a) Short stature, reduced body hair and increased abdominal fat are apparent. (b) Partial breast development results from estrogen replacement. Failure of adrenal androgen production results in the absence of axillary hair. F F Ferri.
Ferri’s color atlas and text of clinical medicine
, 1st edn. Fig 263.2. Saunders, Elsevier, 2009, with permission.
1.
Ask her to stand and make sure she is fully undressed. Note the pale skin and lack of hair.
2.
The patient may be of short stature (failure of growth hormone secretion before growth is complete) with no secondary sexual characteristics (gonadotrophin failure before puberty).
3.
Look at the face more closely. Multiple fine skin wrinkles around the eyes and mouth are characteristic of growth hormone deficiency. Look closely for a hypophysectomy scar on the forehead near the inner canthus of the eye. Examine the eyes for signs of a pituitary tumour (visual fields, especially for bitemporal hemianopia, fundi for optic atrophy) and assess cranial nerves III, IV and VI, as well as the first division of
V (affected by tumour extension into the cavernous sinus). Feel the facial hair over the chin area.
4.
Go to the chest and look for decreased body hair, pale skin and gynaecomastia. Lay the patient down and look for loss of pubic hair and testicular atrophy (in males testes are small and soft – the normal size is 15–25 mL in volume).
5.
Test the ankle jerks (for slow relaxation in hypothyroidism – there is no myxoedematous appearance) and ask to check the blood pressure lying and standing (hypotension with adrenocorticotrophic hormone (ACTH) deficiency).
Cushing’s syndrome
‘This 56-year-old woman has noted weight gain. Please examine her.’
Method (see
Table 16.32
)
This type of introduction may mean Cushing’s syndrome in the clinical examination (
Figs 16.45a–c
). Make sure that the patient is undressed to her underpants and ask her to stand.
Table 16.32
Cushing’s syndrome examination
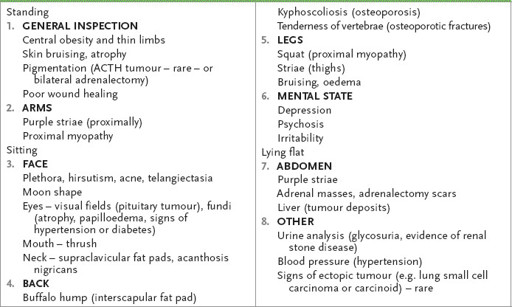

FIGURE 16.45
Cushing’s syndrome (a) Moonface. (b) Buffalo hump. (c) Abdominal striae. C M Townsend.
Sabiston textbook of surgery: the biological basis of modern surgical practice
, 18th edn. Fig 39.11. Saunders, Elsevier 2007, with permission.
1.
Look at the patient from the front, sides and behind. Note central obesity with peripheral sparing and look at the skin for bruising, atrophy and pigmentation of extensor areas. Hyperpigmentation suggests an ectopic ACTH-secreting tumour, or it may indicate an ACTH-secreting pituitary adenoma in a patient who has had a bilateral adrenalectomy (Nelson’s syndrome).
2.
Test for proximal myopathy of the arms and also of the legs (initially by getting the patient to squat). Examine the back for a buffalo hump and feel it. Look for kyphoscoliosis and tap the spine for bony tenderness as a result of osteoporotic vertebral crush fractures.
3.
Ask the patient to sit on the side of the bed. Look at the face for plethora, hirsutism, acne, telangiectasia and a moon shape.
4.
Test the eyes for visual field defects (which are uncommon) and look in the fundi for papilloedema (caused by benign intracranial hypertension or a pituitary tumour) and optic atrophy, as well as hypertensive or diabetic changes (see
Tables 16.7
and
16.41
). Then look at the neck for supraclavicular fat pads and acanthosis nigricans.
Table 16.41
Diabetes mellitus examination
5.
Ask the patient to lie down. Examine the abdomen for adrenalectomy scars, pigmentation, striae and adrenal masses. Look at the genitalia. Virilisation in women or gynaecomastia in men suggests that adrenal carcinoma is more likely. Next look at the legs for oedema, bruising and poor wound healing.
6.
Do not forget to ask for the results of urine analysis (glucose) and take the blood pressure (hypertension). Diagnostic tests are summarised in
Table 16.33
.
Table 16.33
Diagnosis of Cushing’s syndrome
*

To diagnose Cushing’s syndrome, at least two definitive tests should be abnormal
Note:
If Cushing’s disease is present, pituitary assessment is necessary. If adrenal disease is suspected, CT scanning is useful to assess the anatomy. Remember, ectopic ACTH production by a tumour (e.g. small cell carcinoma of lung, carcinoid of lung or thymus, pancreatic islet cell carcinoma, ovarian carcinoma) does not usually cause Cushingoid clinical features but may present with hyperpigmentation, hypokalaemic alkalosis and hypertension.
*
Cushing’s disease is specifically pituitary ACTH overproduction
Acromegaly
‘This 64-year-old man has noted some change in his facial appearance. Please examine him.’ (
Figs 16.46a to c
)

FIGURE 16.46
(a) Acromegalic hands. (b) Macroglossia. (c) This patient has conveniently brought his rings with him.
Method (see
Table 16.34
)
The order and direction of the examination obviously depend on the stem. However, if a ‘change of appearance’ of any part of the body is mentioned in the stem it is likely you are expected to make a spot diagnosis. Look very carefully at the patient before deciding where to examine.
Table 16.34
Acromegaly examination

HINT
The change to a written stem has led to variations on this introduction. At one end of the spectrum the examiners may give the diagnosis: ‘This 64-year-old man has acromegaly. Please examine him to assess the extent and activity of the condition.’ At the other end of the spectrum the introduction may be more oblique: ‘This 64-year-old man has had premature and severe arthritis. Please examine his knees.’
1.
Consider the possible diagnostic facies (see
Table 16.35
). If the patient looks acromegalic, proceed as follows.
Table 16.35
Common diagnostic facies
