i bc27f85be50b71b1 (286 page)
Read i bc27f85be50b71b1 Online
Authors: Unknown
any area above the waisr.)
Duration-Lasts longer than 20 minutes? (Cardiogenic chest pain
typically lasts 2-20 minutes.)

APPENDIX X: PHYSICAL THERAPY CONSIDERATIONS FOR CHEST PAIN 923
Characteristics-Pressure, tightness, or heaviness versus other feelings, such as sharpness, or with inspiration? (Cardiogenic chest pain is usually described as a deep visceral sensation.)
Accompanying symptoms-Associated with diaphoresis, dyspnea, or
light-headedness versus a lack of these symptoms? (Cardiogenic
chest pain is typically associated with one or more of these accompanying symptoms.)
Radiation-Does the pain radiate to the atm(s), shoulder(s), neck,
jaw, or teeth? (Cardiogenic chest pain can radiate widely.)
Treatment-Relieved by rest, oxygen, or nitroglycerin? (Cardiogenic
chest pain is usually relieved by these interventions.)
As this information is ascertained, the physical therapist should
discontinue the activity (if not resting) and determine the need for
seated or supine rest, observe the patient for signs of altered cardiac
output (decreased blood pressure), take vital signs, and monitor
telemetry as appropriate. If the chest pain appeats cardiogenic, the
physical therapist must determine whether it is stable or unstable.
Refer to Myocardial Ischemia and Infarction in Chapter J for a
description of stable, unstable, and variant (Prinzmetal's) angina.
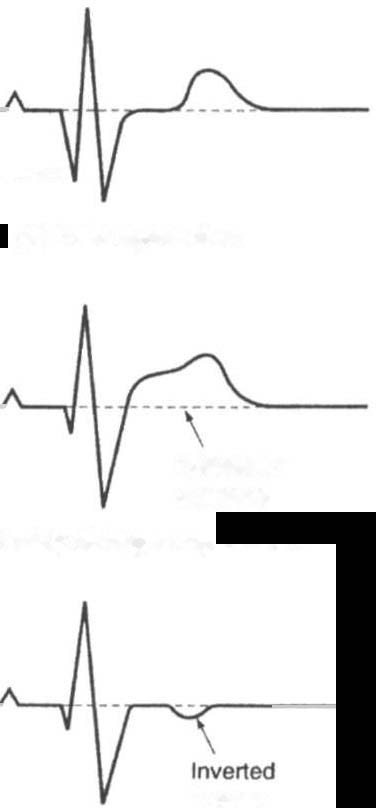
During an episode of unstable angina, an electrocardiograph may
reveal ST segment elevation or depression with or without T-wave
inversion that reverses when anginal pain decreases.4 These electrocardiograph changes are depicted in Figure X-1. Vital sign findings include the following:
•
Hypotension or hypertension
•
Bradycardia Ot tachycardia
•
Irregular pulse
If the patient presents with one or more of these unstable anginal
findings, the therapist should Stop or defer treatment and immediately
notify the nurse.
Regardless of the etiology of the patient's complaint of chest pain,
the physical therapist must be ptepared to expedite a reliable chest pain
description and respond accordingly for prompt medical therapies or
for further investigation of the cause of noncardiogenic chest pain.

924 AClITE CARE HANDBOOK FOR PHYSICAL THERAPISTS
Pathological -
o wave
(a) Dead myocardium
Raised ST
segment
(b) Acutely damaged myocardium
Twave
(c) Myocardial ischemia
Note: There are a range of other
causes for T wave Inversion
Figure X-l. Ischemic electrocardiographic chmJges.
References
1. Becker RC (ed). Chest Pain. Boston: Butterworrh-Heinemann, 2000;40.
2. McAvoy JA. Cardiac pain: discover the unexpected. Nursing 2000;
30:34.
3. Pathophysiology of Coronary Artery Disease. In FJ Brannon, MW Foley,
JA Starr, MG Black (eds), Cardiopulmonary Rehabilitation: Basic Theory
and Application (2nd ed). Philadelphia: FA Davis, 1993;82.
4. Chandra NC. Angina Pcccoris. In LR Barker, PD Burton, PD Ziere (eds),
Principles of Ambulatory Medicine (4th cd). Baltimore: Williams &
Wilkins, 1995;69 t.